3D/4D ultrasound
Gynecology and oncogynecology ultrasound
Generally
These ultrasound examinations are important for clients overcome by clinical gynecological abnormalities and oncogynecological symptoms (uncommon vaginal bleeding, pelvic and abdominal pain, a feeling of pressure in the pelvis, frequent inflammation illnesses, fertility problems and others...) and at the same time who have unclear ultrasound, RTG, CT or MRI findings. Oncogynecological ultrasound is an obligatory examination in the case of suspected malignant gynecological tumour, or with histological verification of a malignant tumours (e.g. excochleation – scraping of the uterine cavity and cervix).
In modern oncogynecology, expert ultrasound is the basic imaging method, as it offers a higher precision than such imaging methods like CT (computed tomography) or MRI (magnetic resonance).
- in the dynamic of the examination and imaging in three dimensions of the given organ
- in the possibility of assessing the mobility of an organ, painfulness, movement of fluid content and elastography
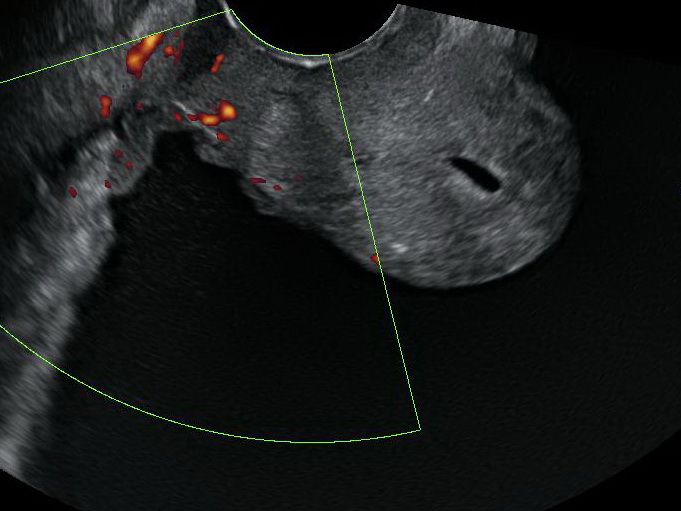
- in the combination of sonographic and flow examination with evaluation of the vascular architecture of a tumour
- in the most detailed imaging of the organs of the pelvis minor
- in the complete absence of ionizing radiation
- in that there is no need for the patient not eating before the examination
When?
The examination is not limited to a certain time period. However, the most optimal time is in the first phase of the menstruation cycle in the case of menstruating girls and women.
How?
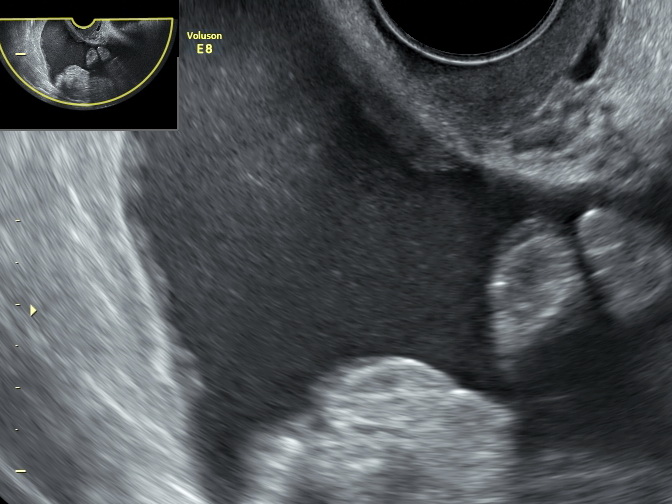
With ultrasound examinations we usually use abdominal or vaginal access.
Abdominal access: a transabdominal probe is placed on the lower abdomen and abdomen of the patient. We typically describe the uterus, ovaries and other organs of the abdomen and pelvis. Describing the pelvic mass, tumours and other abdominal organs may take longer.
Vaginal access: examination by a transvaginal probe enables us to better visualize female sex organs and some organs of the pelvis minor than an abdominal probe. This is due to the closer placing of the probe’s sensor to the examined organs.
Rectal access: a rectal probe, on which a sterile sheath is placed, is sensitively inserted into the rectum. Examination with this type of approach is done with prepubescent girls and those in puberty and with expert oncogynecological ultrasound in the case of cervical carcinoma.
What is it for?
An expert oncogynecological ultrasound consists of an ultrasound examination of the pelvis, abdomen and retroperitoneum with a focus on the local range of the tumour, sentinel nodes and distant metastasis. The examination determines the type and range (clinical staging) of the tumour disease for the necessity of additional therapy or an operation, or another treatment (cytostatic or radiotherapy). Oncogynecological ultrasound with high precision describes the structure, perfusion even in a still non-enlarged node and defines the node as normal, reactive and tumour infiltrated. It thus has an undoubted advantage over CT and MRI (magnetic resonance) examinations in diagnostics of tumour diseases even with non-enlarged nodes. An advantage of ultrasound is also the possible of differentiating viable-living tumour tissue from necrotic-dying tumour tissue and does so thanks to flow examination, which is based on the detection of newly created blood vessels in the tumour.
- local range of disease, including invasion to surrounding structures (stadium T)
- state of the lymphatic nodes (stadium N)
- presence of distant metastasis (stadium M)
T: When assessing the local finding of a tumour disease, we focus on its extent, infiltration into the surrounding vaginal connective tissue, cervix and the uterus. With a local advanced disease in the pelvis, we also assess the spread of the tumour to the surrounding structures – most often in the rectum (anus) and the urinary bladder. We describe the structure of the kidneys, or possible implantation metastasis (carcinomatosis) of the peritoneum (peritoneal membrane).
N: Oncogynecological ultrasound accurately describes the structure, perfusion and non-enlarged nodes and evaluates the nodes as normal, reactive and tumour infiltrated. This has an unquestionable advantage over CT and MRI scans in the diagnosis of tumour diseases, even in non-enlarged nodes. We evaluate peripheral, retroperitoneal and visceral nodes.
M: When evaluating distant metastases, we focus systematically on individual parenchymatous organs of the abdominal cavity, such as the liver, spleen, kidneys, adrenals and pancreas.
| USG staging | Sensitivity % | Specificity % |
|---|---|---|
| Cervical neck carcinoma | 84 | 91 |
| Uterine body carcinoma | 85-100 | 65-80 |
| Ovarian carcinoma | 90 | 90 |
| USG of the kidneys | 76,5 | 100 |
| USG of the liver | 61 | 80 |
| USG lymphadenopathy - retroperitoneum | 67 | 78 |
| USG lymphadenopathy - of the groin, inguinal | 86 | 96 |
| USG staging | presnosť USG | presnosť MRI |
|---|---|---|
| Detection of carcinoma > 1cm | 94% | 83% |
| Detection of carcinoma < 1cm | 91% | 81% |
| Disability of parameters | 97% | 86% |
| Sensitivity | 68 – 93% |
|---|---|
| Specificity | 82 – 83% |
| Tendency to over evaluate the depth of the myometrial invasion | In cases of more than 50% width of the myometria |