Pregnancy consulting
Screening for preeclampsia
Generally
Preeclampsia (PE) occurs globally in 3 to 14% of pregnancies. The incidence of preeclampsia in Europe ranges from 4 to 8%. The perinatal mortality with preeclampsia ranges from 4 to 28% and the prematurity caused by preeclampsia ranges from 15 to 40%. This pregnancy-specific disease results in multi-organ damage to the mother, primarily occurring in the kidneys, liver, brain, lungs, placenta, blood-forming system and blood vessels. The clinical symptoms of preeclampsia begin to manifest almost always after the 20th week of pregnancy. Ultrasound examination together with placental hormone testing is currently the only way of determining the risk of developing preeclampsia in the first or second trimester of the pregnancy. Early detection of a high risk of developing preeclampsia allows us to take action and prevent the development of this disease.
- Early-onset preeklampsia occurs up to the 34th week of pregnancy, due to placental endothelial disorder
- Late-onset preeklampsia occurs in and after the 34th week of pregnancy due to a deficiency of the mother's cardiovascular system
- Definition of mild preeclampsia - hypertension at rest (systolic blood pressure > 140 mmHg or diastolic blood pressure > 90 mmHg), protein occurrence in the urine (300 mg or more per 24 hours) and lower limb swelling.
- Definition of severe preeclampsia - hypertension with systolic blood pressure ≥ 160 mmHg and diastolic blood pressure ≥ 1140 mmHg, high degree of occurrence of protein in the urine (2.0 g per 24 hours or protein at +++ / 3 crosses in the indicator test), swollen limbs and other body parts. Serious preeclampsia is also defined by the development of mild preeclampsia symptoms prior to the 34th week of pregnancy. Severe preeclampsia occurs in 25% of women with preeclampsia
- It may manifest at any time after 20 weeks of pregnancy
- Initial pathological changes occur in the placenta already in the first trimester
- Severe preeclampsia may also have further manifestations of the disease in the mother (pulmonary oedema, liver and kidney failure, cerebral haemorrhage, placental abruption, seizures, and rarely death of the mother) and the foetus (premature birth, growth retardation, foetal death)
When?
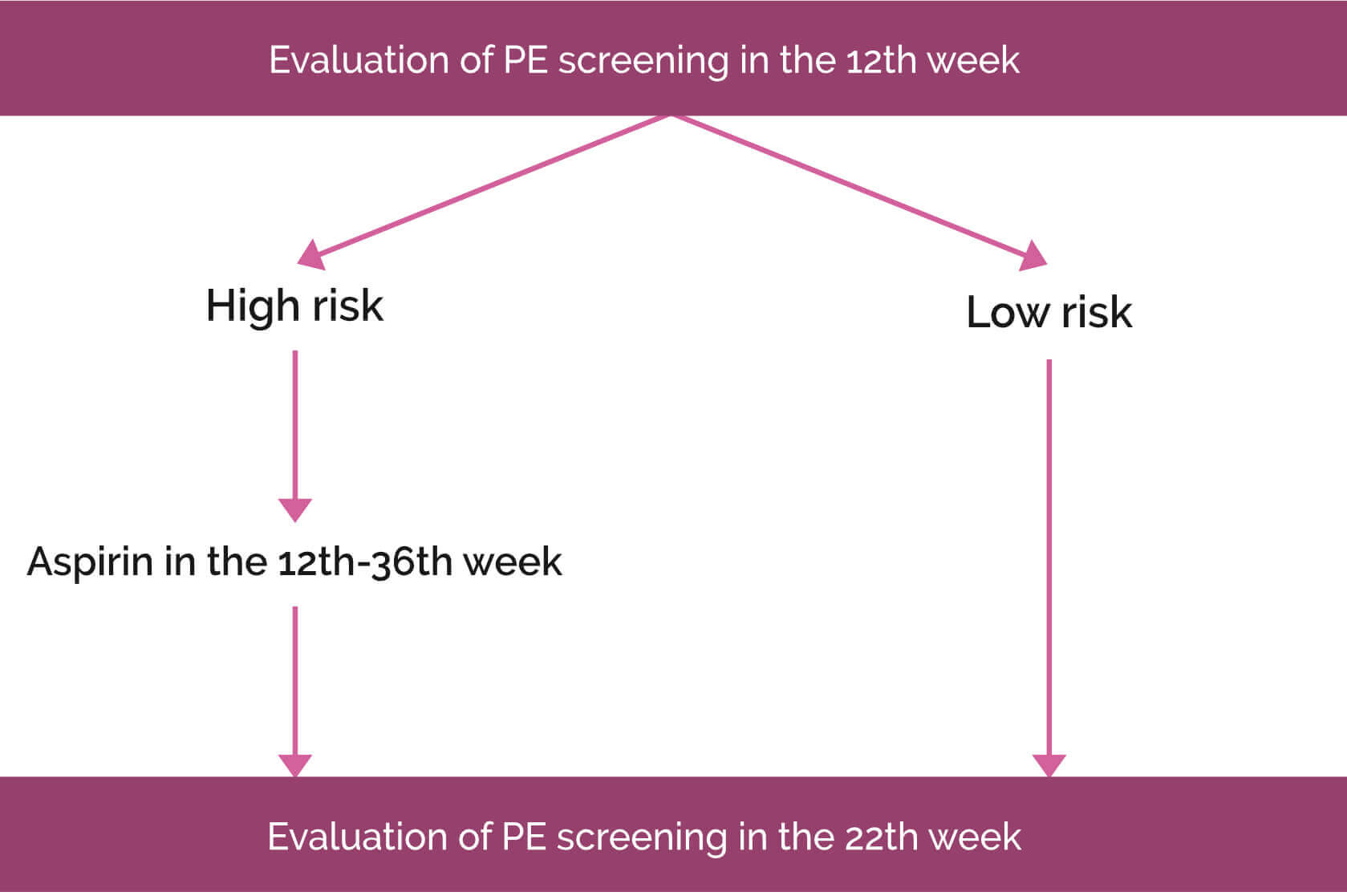
Preeclampsia screening is performed during the first trimester with the ultrasound examination and the combined test at 12-14 weeks of pregnancy, and then after the 20th week of pregnancy during the second and third trimester.
METHOD OF PREECLAMPSIA
SCREENING IN 11-13 WEEKS OF PREGNANCY

| Preeclampsia before the 34th week of pregnancy | Preeclampsia before the 37th week of pregnancy | Preeclampsia in and after the 37th week of pregnancy | |
|---|---|---|---|
| - Pacientkine faktory | 58% | 50% | 38% |
|
- Patient factors - Measuring of central arterial pressure | 65% | 60% | 43% |
|
Kombinovaný test: - Patient factors - Measuring of central arterial pressure - USG meranie maternicových tepien - Blood examination for placental hormone PLGF | 80% | 70% | 44% |
|
- Patient factors - Measuring of central arterial pressure - USG meranie maternicových tepien - Krvné vyšetrenie placentárneho hormónu PLGF a sFlt-1 | 90% | 75% | 47% |
METHOD OF PREECLAMPSIA
SCREENING IN 20 - 24 WEEKS OF PREGNANCY

| Preeclampsia before the 34th week of pregnancy | Preeclampsia before the 37th week of pregnancy | Preeclampsia in and after the 37th week of pregnancy | |
|---|---|---|---|
| - Patient factors | 52% | 47% | 36% |
|
- Patient factors - Measuring of central arterial pressure | 72% | 60% | 44% |
|
- Patient factors - Measuring of central arterial pressure - Krvné vyšetrenie placentárneho hormónu PLGF a sFlt-1 | 94% | 85% | 45% |
|
- Patient factors - Measuring of central arterial pressure - USG meranie maternicových tepien pri morfologickom vyšetrení plodu | 96% | 80% | 44% |
|
- Patient factors - Measuring of central arterial pressure - Krvné vyšetrenie placentárneho hormónu PLGF a sFlt-1 - USG meranie maternicových tepien pri morfologickom vyšetrení plodu | 100% | 85% | 45% |
METHOD OF PREECLAMPSIA
SCREENING IN 30 - 34 WEEKS OF PREGNANCY

| Preeclampsia before the 37th week of pregnancy | Preeclampsia in and after the 37th week of pregnancy | |
|---|---|---|
| - Patient factors | 34% | 30% |
|
- Patient factors - Measuring of central arterial pressure | 79% | 39% |
|
- Patient factors - Measuring of central arterial pressure - USG measuring of uterine pulse during so-called “USG examination of flows” | 79% | 40% |
|
- Patient factors - Measuring of central arterial pressure - USG measuring of uterine pulse during so-called “USG examination of flows” - Krvné vyšetrenie placentárneho hormónu PLGF a sFlt-1 | 98% | 55% |
How?
We perform ultrasound examination in the first trimester by visualizing both uterine arteries (uterinae), in which we examine the Doppler metric blood flow. Subsequently, the combined test determines the risk of preeclampsia by using ultrasound, the medical history of the patient and placental hormone values. Patients with a high risk for the possible development of preeclampsia are advised prophylactic therapy in the form of low-dose acetylsalicylic acid. At the same time, these patients undergo a second-stage screening of preeclampsia after the 20th week of pregnancy in the form of pomer-biochemical markers sFlt1/PlGF.


What is it for?
Early screening and detection of preeclampsia allow us to successfully influence the development and heal the consequential multiple organ damage of the mother and the foetus. Each patient should know her degree of the risk for preeclampsia from the first-trimester combined test. This is of the utmost importance for the outcome of prophylactic treatment with acetylsalicylic acid, since its onset administration after 17th week of pregnancy does not have an adequate effect.