Pregnancy consulting
Screening for premature birth
Generally
Preterm birth is defined as a delivery before the 37th week of pregnancy. Preterm birth occurs in 7 to 10% of pregnancies. The worst complications, such as severe neurological-somatic damage to the new-born or its death, are the results of a delivery before the 32nd week of the pregnancy. In repeated figures this means approximately 2 to 3% of all pregnancies. Over the last 50 years, the number of preterm births has not changed. Because of this fact, we looked for the best screening exam as early as possible in the lower weeks of pregnancy for the greatest possible identification of women who may be at risk of preterm birth and who are still without clinical symptoms.
Vaginal examination (palpation), expressed in the so-called cervix score (Bishop's score), fails to catch early changes in the cervix. It also fails to accurately describe the more advanced changes leading to premature birth. The basic difference between ultrasound and palpation examination is that ultrasound can describe cervical changes as an anatomical structure, whereas palpation examination is much more limited.
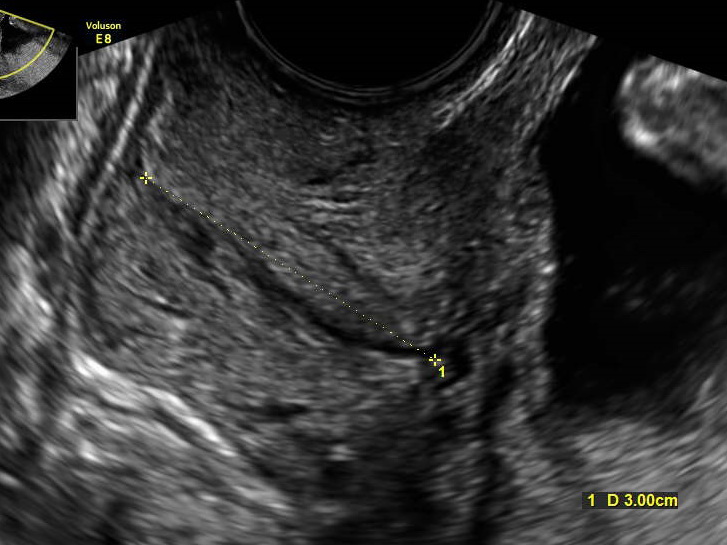
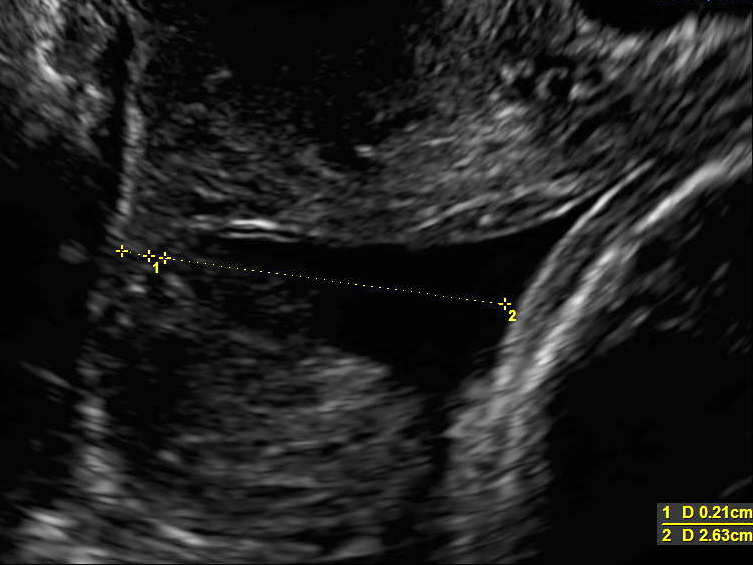
Currently, the best method of predicting preterm birth is ultrasound examination of the length of the cervical canal with its elastography and examination of decidual proteins in the vaginal secretion via bedside rapid tests (fibronectin or phosphorylated insulin-like growth factor binding protein). With this ultrasound examination we can direct the pregnant woman in time to a surgical procedure on the uterine cervix - cerclage, for progesterone therapy. In the long term, an ultrasound examination of the cervix was unable to express its assessment of the consistency-stiffness, as in the palpation vaginal examination. The given disadvantage of ultrasound examination under the guidance of a new ultrasound modality – ELASTOGRAPHY – has been removed. Thanks to this, we can objectively evaluate the consistency of individual parts of the cervix and cervical canal in its entire anatomical structure.
When?
Screening for premature birth is performed from the 12th week of pregnancy during the combined test. With high precision, it selects a group of patients a positive risk of premature birth. These include, in particular, patients with a history of pregnancy after two or more abortions, pregnancy after surgery on the cervix, such as cerclage and conization, pregnancies after pre-term delivery/-ies, and women with a risky family history. In this group of patients, we recommend a follow-up examination of the length and elastography of the cervical canal from 15th to 34th weeks of pregnancy. Thanks to the follow-up measurements, we can define whether the inner neckline of the cervix changes and whether the cervix is progressively shortening, and thus schedule a timely and effective therapy for the threat of premature birth. Incompetence of the cervix often manifests itself without other symptoms, that is, it is asymptomatic. The mentioned screening from the 22nd week of pregnancy is complemented by bedside tests of decidual proteins, which all in all express the possibility of premature delivery within the 7-day horizon and thus require hospitalization.
How?
We perform the examination with a vaginal ultrasound probe and calculation of the risks for premature birth by software conversion after counting other anamnestic data (age, pregnancy week in previous pregnancies if there were any) based on the results of the most recent multicentre studies. After the result of the test, a further procedure with an optional bed-side rapid test to detect the presence of the decidual (placental) protein is suggested and explained.
What is it for?
Skríning predčasného pôrodu je dôležitou súčasťou prenatálnych poradní v tehotenstve. Umožňuje najmä záchyt skupiny žien, ktorej včasnou progesterónovou terapiou eventuálne chirurgickým zásahom sme schopní oddialiť pôrod na nevyhnutný čas. Tento včasný záchyt sa uskutočnuje už začiatkom druhého trimestra a teda posúva hranicu objektívneho rozhodovania sa o niekoľko gestačných týždňov skôr ako pri palpačnom vaginálnom vyšetrení! Ultrazvukové vyšetrenie cervixu ako skríning predčaného pôrodu nielenže plne nahrádza palpačné vyšetrenie, ale ho aj významne predbieha čo sa týka presnosti hodnotenia a včasnosti záchytu rozvoja predčasného pôrodu. Vyšetrenie zachytáva aj významnú skupinu žien, ktoré subjektívne nepociťujú a neudávajú kontrakcie “tvrdnutie” bruška. Teda ženy, ktoré sú asymptomatické a bez tohto vyšetrenia by účinnému zabráneniu predčasnému pôrodu nebolo možné. V neposlednom rade celkovému manažmentu takýchto gravidít významne napomáha aj detekcie placentárnych proteínov v cervikálnom sekréte, ktoré s vysokou negatívnou prediktívnou hodnotou upozorňujú na prípadnú možnosť pôrodu do 7 dní od realizovaného vyšetrenia.