3D/4D ultrasound
Ultrasound in gynecology
At CFGD we offer complete diagnostic care in the field of routine gynecological diseases, sterility, infertility, oncogynecology and pediatric gynecology. Each year we catch several dozen oncogynecology diseases, congenital developmental defects of genitourinary tract and tubal sterilities with extensive endometriosis process.
Ultrasound in gynecology
At CFGD we offer complete diagnostic care in the field of routine gynecological diseases, sterility, infertility, oncogynecology and pediatric gynecology. Each year we catch several dozen oncogynecology diseases, congenital developmental defects of genitourinary tract and tubal sterilities with extensive endometriosis process.
Gynecology and oncogynecology ultrasound
Generally
These ultrasound examinations are important for clients overcome by clinical gynecological abnormalities and oncogynecological symptoms (uncommon vaginal bleeding, pelvic and abdominal pain, a feeling of pressure in the pelvis, frequent inflammation illnesses, fertility problems and others...) and at the same time who have unclear ultrasound, RTG, CT or MRI findings. Oncogynecological ultrasound is an obligatory examination in the case of suspected malignant gynecological tumour, or with histological verification of a malignant tumours (e.g. excochleation – scraping of the uterine cavity and cervix).
In modern oncogynecology, expert ultrasound is the basic imaging method, as it offers a higher precision than such imaging methods like CT (computed tomography) or MRI (magnetic resonance).
- in the dynamic of the examination and imaging in three dimensions of the given organ
- in the possibility of assessing the mobility of an organ, painfulness, movement of fluid content and elastography
- in the combination of sonographic and flow examination with evaluation of the vascular architecture of a tumour
- in the most detailed imaging of the organs of the pelvis minor
- in the complete absence of ionizing radiation
- in that there is no need for the patient not eating before the examination
When?
The examination is not limited to a certain time period. However, the most optimal time is in the first phase of the menstruation cycle in the case of menstruating girls and women.
How?
With ultrasound examinations we usually use abdominal or vaginal access.
Abdominal access: a transabdominal probe is placed on the lower abdomen and abdomen of the patient. We typically describe the uterus, ovaries and other organs of the abdomen and pelvis. Describing the pelvic mass, tumours and other abdominal organs may take longer.
Vaginal access: examination by a transvaginal probe enables us to better visualize female sex organs and some organs of the pelvis minor than an abdominal probe. This is due to the closer placing of the probe’s sensor to the examined organs.
Rectal access: a rectal probe, on which a sterile sheath is placed, is sensitively inserted into the rectum. Examination with this type of approach is done with prepubescent girls and those in puberty and with expert oncogynecological ultrasound in the case of cervical carcinoma.
What is it for?
An expert oncogynecological ultrasound consists of an ultrasound examination of the pelvis, abdomen and retroperitoneum with a focus on the local range of the tumour, sentinel nodes and distant metastasis. The examination determines the type and range (clinical staging) of the tumour disease for the necessity of additional therapy or an operation, or another treatment (cytostatic or radiotherapy). Oncogynecological ultrasound with high precision describes the structure, perfusion even in a still non-enlarged node and defines the node as normal, reactive and tumour infiltrated. It thus has an undoubted advantage over CT and MRI (magnetic resonance) examinations in diagnostics of tumour diseases even with non-enlarged nodes. An advantage of ultrasound is also the possible of differentiating viable-living tumour tissue from necrotic-dying tumour tissue and does so thanks to flow examination, which is based on the detection of newly created blood vessels in the tumour.
- local range of disease, including invasion to surrounding structures (stadium T)
- state of the lymphatic nodes (stadium N)
- presence of distant metastasis (stadium M)
T: When assessing the local finding of a tumour disease, we focus on its extent, infiltration into the surrounding vaginal connective tissue, cervix and the uterus. With a local advanced disease in the pelvis, we also assess the spread of the tumour to the surrounding structures – most often in the rectum (anus) and the urinary bladder. We describe the structure of the kidneys, or possible implantation metastasis (carcinomatosis) of the peritoneum (peritoneal membrane).
N: Oncogynecological ultrasound accurately describes the structure, perfusion and non-enlarged nodes and evaluates the nodes as normal, reactive and tumour infiltrated. This has an unquestionable advantage over CT and MRI scans in the diagnosis of tumour diseases, even in non-enlarged nodes. We evaluate peripheral, retroperitoneal and visceral nodes.
M: When evaluating distant metastases, we focus systematically on individual parenchymatous organs of the abdominal cavity, such as the liver, spleen, kidneys, adrenals and pancreas.
| USG staging | Sensitivity % | Specificity % |
|---|---|---|
| Cervical neck carcinoma | 84 | 91 |
| Uterine body carcinoma | 85-100 | 65-80 |
| Ovarian carcinoma | 90 | 90 |
| USG of the kidneys | 76,5 | 100 |
| USG of the liver | 61 | 80 |
| USG lymphadenopathy - retroperitoneum | 67 | 78 |
| USG lymphadenopathy - of the groin, inguinal | 86 | 96 |
| USG staging | presnosť USG | presnosť MRI |
|---|---|---|
| Detection of carcinoma > 1cm | 94% | 83% |
| Detection of carcinoma < 1cm | 91% | 81% |
| Disability of parameters | 97% | 86% |
| Sensitivity | 68 – 93% |
|---|---|
| Specificity | 82 – 83% |
| Tendency to over evaluate the depth of the myometrial invasion | In cases of more than 50% width of the myometria |










HyCoSy and HSN
Generally
Infertility affects approximately 10% of couples in modern developed countries. From 20 to 40% of them are the result of abdominal operations or after overcoming infections of the fallopian tubes, but which the patient does not necessarily know about. With respect to this diagnostic management leans in the first step towards minimal invasiveness and not to an immediate surgical intervention! Many works have been published, especially in Germany, the UK, the USA and Australia, confirming the comparable results of HyCoSy (Hysterosalpingo-contrast-sonography) with x-ray hysterosalpingography and laparoscopy. Therefore, HyCoSy in modern gynecological diagnostics is the first choice with suspected impassability of the fallopian tubes and is considered to be the gold standard.
As with other imaging techniques even with ultrasound it isn’t possible to see everything and this imaging method also has its limitations. Sometimes instilling the gel into the cavity of the uterus - hysterosonography HSN helps us overcome these limitations and improves the imaging of the endometrium (the uterine lining), on which polyps or other serious pathological changes can be identified.
When?
We carry out both diagnostic modalities most often in the follicular phase of the menstruation cycle, i.e. in the first 10 to 14 days. HSN also becomes and obligatory examination in the planning of reproduction of the mother after two Caesarean sections.
How?
HyCoSy (so-called HyFoSy) is a contrasting transvaginal ultrasound technique, during which we use a contrasting gel/foal (ExEm Foam®), where the passage of this gel through the fallopian tubes is observable under ultrasound and subsequently evaluated. With ultrasound examinations of the passability of the fallopian tubes we use 2D and 3D/4D imaging.

Hysterosonography – HSN is a new technique, created for better ultrasound imaging of the uterine cavity. A sterile gel is applied using a soft plastic catheter placed in the cervix. The gel expands the cavity and enables it to be much better imaged by the transvaginal ultrasound. This technique is used for assessing CBD and other abnormalities of the uterus and endometrium.

What is it for?
The advantages and safety of HyCoSy are now in the front line of examination of female infertility and thus it is preferred over x-ray hysterosalpingography and laparoscopy. HyCoSy also enables examination of other pelvic organs, and therefore it is a dynamic examination that offers valuable information about functioning of the fallopian tubes. The first advantage of HyCoSy is that the client doesn’t have to undergo any hospitalization, as with x-ray hysterosalpingography or laparoscopy. A client during HyCoSy is not exposed to x-ray ionizing radiation in the area of the pelvis minor and especially the ovaries as with x-ray hysterosalpingography, where the possibility also exists of development of acute allergic reaction to x-ray contrast medium. HyCoSy versus laparoscopy does not require any form of anaesthetic and at the same time with laparoscopy a single-day or longer term hospitalization is required. Laparoscopy as well as other operations bear in themselves the risk of a surgical intervention and anaesthesia itself. Sometimes, however, the same important diagnostic cannot be avoided.

A lot of women experience unusual bleeding especially during menopause. This is often a consequence of hormonal changes, where an operation (excochleation, hysteroscopy) has a very few benefits. Therefore, if HSN does not display an evident problem in the uterine cavity, further examination (excochleation, hysteroscopy, etc.) is not necessary. Sometimes with standard gynecological ultrasound the uterine mucosa appears normal, but during HSN we see polyps or another organic change. The most common findings are polyps of the endometrium, myoma, endometrial hyperplasia and adenomyosis. HSN with causes of infertility and repeating miscarriages can diagnose growths, polyps of the mucosa or lining defects of the uterus, which can prevent pregnancy occurring. It evaluates in detail the uterine mucosa in patients with tamoxifen treatment for breast cancer. HSN is an essential examination for the evaluation of the quality of the uterine “scar” after two or more Caesarean sections in clients planning further reproduction.






Ultrasound with infertility and PCOs
Generally
- Disorders of ovulation
- Polycystic ovary syndrome – PCOS
- Tubal infertility
- Problems with the uterus
- Age of the woman and quality of the eggs themselves
- Unexplained infertility
- Male infertility
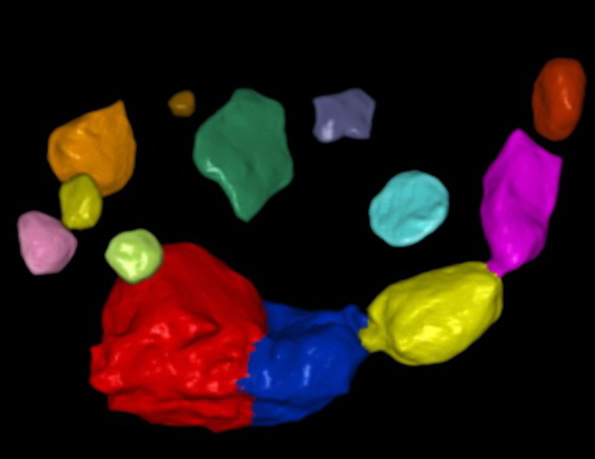
The purpose of a Sono AVC ultrasound examination of the ovarian reserve is to determine the number of follicles in the ovaries and to identify women with an ovarian reserve (AFC <3-10) and women with polycystic ovaries. Thanks to this procedure we are able to identify women with a favourable prognosis and women with a reduced probability of spontaneous pregnancy.
| Number of antral follicles | Number of years to last possible pregnancy | Number of years to menopause |
|---|---|---|
| 20 | 14,8 | 24 |
| 12 | 9,3 | 18,4 |
| 10 | 4,2 | 12,9 |
| 5 | 0 | 7,3 |
Evaluation of ovulation is an important part of each examination in the scope of a menstruation cycle disorder. Even though regular menstruation cycles point to normal ovulation, this is not always the case.
Normal ovulation of a woman requires the interaction of several factors, such as correctly timing of levels of individual hormones up to the ovarian reserve itself. Often a small hormonal imbalance or disorder of ovulation can lead to “suboptimal fertility potential” i.e. subfertility.
- Inadequate ovulation
- Preliminary luteinized follicle
- Luteinized unruptured follicle (LUF syndrome)
- Insufficient luteal phase
- Lowered ovarian reserve
- Transvaginal pelvic ultrasound examination
- Measuring of basal body temperature (BBT)
- LH tests
- Biopsy of the endometrium
- Blood examinations of hormones (TSH, prolactin, total and free testosterone, DHEA, DHEAS, SHBG, AMH....)
- Vyšetrenia ovariálnej rezervy (AMH blood level, veľmi raritne každý cyklus na 3 deň FSH/ESTRA alebo clomid challenge test – CCCT)
When?
We determine the type of ovulation disorder and PCOS on the basis of wide hormonal profiles and ultrasound folliculometric measurement (AFC). Therefore, we plan the approach to each woman individually with regard to her menstruation cycle. We usually perform ultrasound examination focused on ovulation disorders (AFC) in 2 daily intervals from about the 9th day of the menstruation cycle from the first day of bleeding.
How?
The examination is performed by a vaginal ultrasound probe and lasts from 5 to 10 minutes. The numbers, absolute sizes and volumes of the follicles are subsequently evaluated very precisely using an expert software program. 3D ultrasound mapping is the most ideal tool for evaluation of the ovaries and their follicles in women with ovulation disorders and undergoing induction. For the most exact findings of the number of antral follicles we offer an expert 3D methodology determining their number and size: Sono AVC (Automatic Volume Calculation from GE Medical systems).
What is it for?
Previously, only conventional 2D ultrasound was used to determine the size of follicles, but this only gave the real volume of the follicles and an exact time of ovulation could only be estimated. The results of comparative studies have shown that using the new 3D method of Sono AVC in comparison with 2D ultrasound measurement significantly more eggs mature in the course of induction. The 3D ultrasound Sono AVC method is therefore much more objective, faster and reliable and displays the follicle metric reality much more precisely than common 2D ultrasound measurement. This leads to optimal adaptation of the entire process of stimulation and induction of ovulation in the sense of improved quality according to the aims of Directive 2004/23/EC of the European Parliament and of the Council of 31 March 2004).
The aim of stimulation and induction of ovulation is the production of a larger number of follicles in the ovaries, each of which contains an egg-oocyte and subsequently ensure its release, or “rupturing” of the dominant follicle. A month before the planned induction of ovulation, we can apply hormonal anticonception on a client as a gentle prevention of the creation of ovarian cysts. These cysts, which commonly occur in patients before the use of peroral anticonception, hold back the start of the cycle with an intervention into the normal hormonal function of the ovary.
For patients in whom before and during stimulation of ovulation we carry out 3D Sono AVC measurements, we demonstrably determine the following results:
- Higher number of qualitative follicles (criterial according to L. Veek)
- Higher success rate of impregnation with determined ovulation
- Significantly lower occurrence of ovarian hyperstimulation syndrome (OHSS)
With the help of correct management and treatments of certain ovulation disorders, adequate ovulation can be achieved in harmony with the menstruation cycle and subsequently possible pregnancy. It is especially important to point out the necessity of the ovarian reserve by a method of counting antral follicles in women with a diagnosis of polycystic ovaries (PCO).