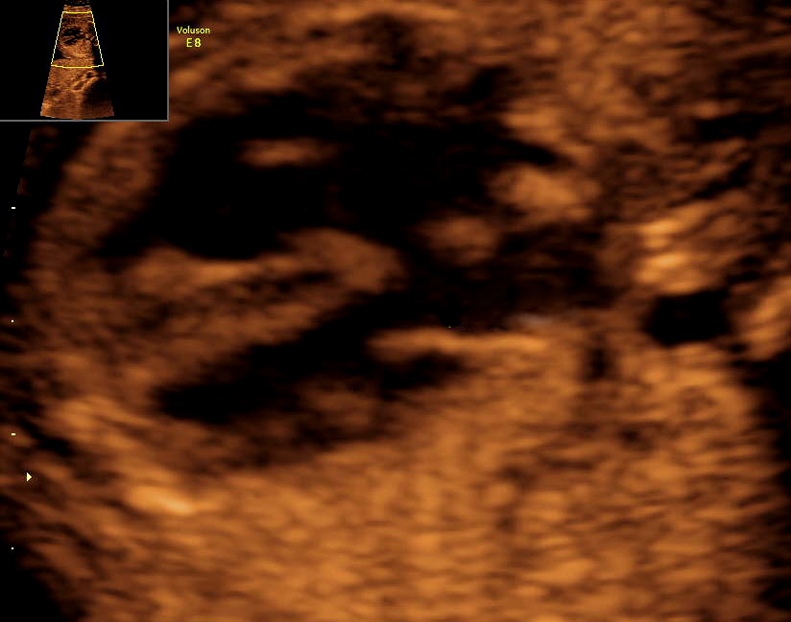
3D/4D ultrasound
VIABILITY SCAN
Generally
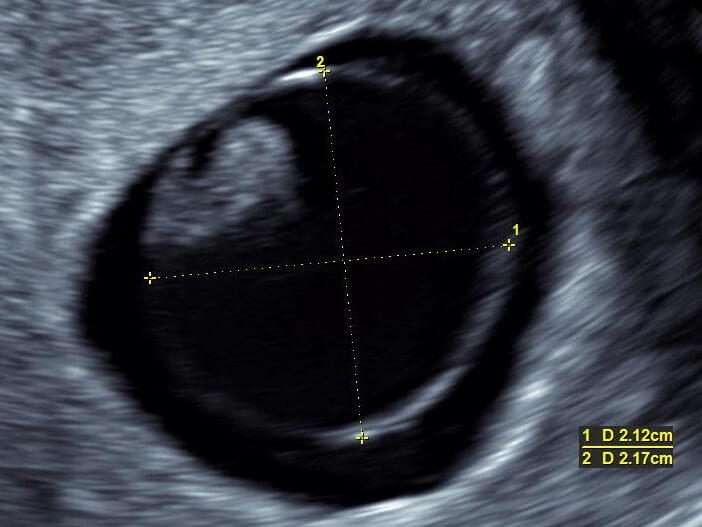
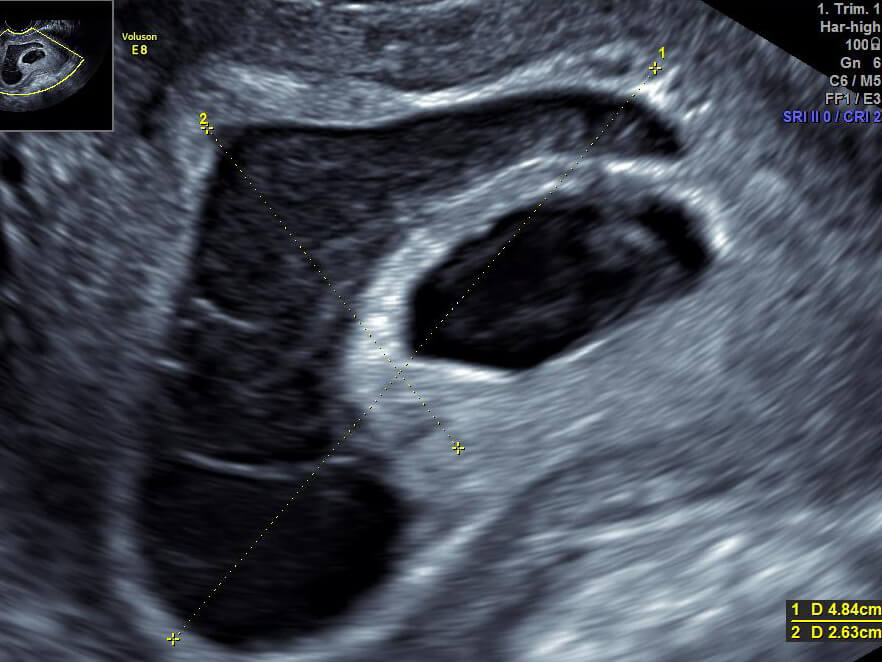
The aim is to confirm the presence of an embryo in the uterus and to exclude the possibility of an ectopic pregnancy in the 6th week of pregnancy. The examination also determines the number of embryos, the vitality, the exact length of the current pregnancy and evaluates anomalies of the uterus, ovaries, fallopian tubes and possible risk symptoms of miscarriage.
When?
We perform a viability scan at the start of the 1st trimester of pregnancy (between the 6th and 11th week). Ultrasound visualization and the beginning of an intrauterine pregnancy is possible as early as in the 5th week, i.e. on about the 26th to 31st day from the first day of the last menstruation or according to the hCG blood values.
| Phases of the 1st trimester | Week of gestation |
|---|---|
| Pre-embryonal | 3 |
| Embryonal | 4 – 10 |
| Foetal | 11+ |
How?
We perform the examination intravaginally using an ultrasound probe, for a much more precise visualization and description of the beginning pregnancy.
What is it for?
- we realistically determine the viability of the pregnancy and its localization
- the activity of the primitive heart can be depicted by the end of the 6th week with an embryo length of about 3-4 mm and can be demonstrable at the latest by the end of the 7th week of pregnancy
- in the course of the 9th week of pregnancy a second sign of vitality of the embryo is found, and this is its movements
- from the 9-11th week of pregnancy we determine the so-called CRL (crown-rump length) of the embryo. This is the period most optimal for measuring the CRL and in this way estimating as exactly as possible the due date of birth (deviation +/-4.7 days)


On the basis of certain values of heart of frequency before the 8th week of pregnancy, early visualization of the amniotic sac still before the 7mm size of the embryo and non-correlation diameter of the size of the vitelline sac we can determine a certain percentage prediction of possible early loss of pregnancy - miscarriage. To counter the so-called prediction of possible miscarriage we also add an evaluation of the origin of a peri ovular event, a retrochorial haematoma.


Jedna zo základných odpovedí, ktoré by mali byť zodpovedané do konca 7 týždňa gravidity je chorionicita v prípade viacplodovej gravidity (dvojčatá, trojčatá…), tzn. vyjadrenia sa k budúcemu vytvoreniu jednej spoločnej, alebo viacerých samostatných placent.
VIABILITY SCAN
Generally
The aim is to confirm the presence of an embryo in the uterus and to exclude the possibility of an ectopic pregnancy in the 6th week of pregnancy. The examination also determines the number of embryos, the vitality, the exact length of the current pregnancy and evaluates anomalies of the uterus, ovaries, fallopian tubes and possible risk symptoms of miscarriage.
When?
We perform a viability scan at the start of the 1st trimester of pregnancy (between the 6th and 11th week). Ultrasound visualization and the beginning of an intrauterine pregnancy is possible as early as in the 5th week, i.e. on about the 26th to 31st day from the first day of the last menstruation or according to the hCG blood values.
| Phases of the 1st trimester | Week of gestation |
|---|---|
| Pre-embryonal | 3 |
| Embryonal | 4 – 10 |
| Foetal | 11+ |
How?
We perform the examination intravaginally using an ultrasound probe, for a much more precise visualization and description of the beginning pregnancy.
What is it for?
- we realistically determine the viability of the pregnancy and its localization
- the activity of the primitive heart can be depicted by the end of the 6th week with an embryo length of about 3-4 mm and can be demonstrable at the latest by the end of the 7th week of pregnancy
- in the course of the 9th week of pregnancy a second sign of vitality of the embryo is found, and this is its movements
- from the 9-11th week of pregnancy we determine the so-called CRL (crown-rump length) of the embryo. This is the period most optimal for measuring the CRL and in this way estimating as exactly as possible the due date of birth (deviation +/-4.7 days)
On the basis of certain values of heart of frequency before the 8th week of pregnancy, early visualization of the amniotic sac still before the 7mm size of the embryo and non-correlation diameter of the size of the vitelline sac we can determine a certain percentage prediction of possible early loss of pregnancy - miscarriage. To counter the so-called prediction of possible miscarriage we also add an evaluation of the origin of a peri ovular event, a retrochorial haematoma.
Jedna zo základných odpovedí, ktoré by mali byť zodpovedané do konca 7 týždňa gravidity je chorionicita v prípade viacplodovej gravidity (dvojčatá, trojčatá…), tzn. vyjadrenia sa k budúcemu vytvoreniu jednej spoločnej, alebo viacerých samostatných placent.
I. trimester
Combined test
Generally
Every pregnant woman has a certain risk of possible disability of a foetus with a chromosomal abnormality. This risk in general is increased with the age of the mother and is lowest at the time of birth in 20-year-old women (1:1500) and at its highest in 50-year-old women (1:5). Even though the risk of Down Syndrome (trisomy 21) in a foetus in the group of women ≥35 years old is higher, most foetuses with Down Syndrome occur in the group of women 25 to 30 years old. This is due to the number of this group in the scope of the overall population of pregnant women. In the population of women ≥35 years old, around 30% of all children would be born with Down Syndrome if there was no screening done. Trisomy 21 is manifested by mental and physical disability of the individual in many variants and ranks among the most common chromosomal aberrations (more at: wikisripta.eu/downůvsyndrom and downovsyndrom.sk).
The combined test is first-trimester screening for trisomy 21 and other chromosomal aberrations, such as Edwards and Patau syndrome (trisomy 18 and 13, respectively). A positive test for a chromosomal aberration at the same time predicts the risk for up to 200 other possible genetic syndromes. The mentioned patient screening also determines the risks for preeclampsia, growth retardation of the foetus and premature birth.
A part of the test is the ultrasound measuring of NT (nuchal translucency). Due to its high detectability (95-98%) and low false positive (2-3%) it is the first choice in all leading world foetal centres. With screening we also determine the exact time of birth using the ultrasound CRL measurement (crown-rump length) with precision to +/- 5 days.
Unfortunately, in Slovakia during this period only biochemical screening in the 2nd trimester is for the most part represented. Its disadvantage compared to the combined test is its low 60-65% detectability for trisomy 21 and others, with a probability of 5-10% false positive.
In our centre we perform a single-step multiple marker combined test and not an integrated test, because the integrated test doesn’t enable us to tell a patient the result of the test while still in the 1st trimester, given that a part of the biochemical sampling and the overall calculation of risks for chromosomal aberrations is done only in the 2nd trimester. Pri kombinovanom teste pacientka dostáva výsledok už v I. trimestri a vďaka tomu je odbúraný stres z čakania na výsledok.
When?
The combined test is done in the 11+0 – 13+6 weeks of pregnancy (i.e. weeks 12-14), that is with the CRL size of the foetus from 45 to 84 mm. It is best to schedule the given test after confirmation and dating of pregnancy by your primary gynecologist.
How?

- Medical history data, i.e. data on your age, height, weight, method of conception, race, chronical diseases, etc…. The client fills in the given data into a questionnaire in informed consent.
- Blood sampling for determining the values of free ß-hCG and PAPP-A from blood serum of the pregnant woman, for which you need not come on an empty stomach.
- Ultrasound examination of the foetus consisting of NT measuring, evaluation of the presence of nasal bones (NB), from measuring the blood flow through the ductus venosus (DV, the body vein) and through tricuspid valve (TR, evaluates the incompetence of the tricuspid valve). We also examine the early morphology of the foetus with a focus on its possible abnormality. We are capable of detecting up to 75% of foetal abnormalities in the 1st trimester. The following have a high percentage of detectability, e.g.: diaphragmatic hernia, skeletal dysplasia of the limbs, large heart defects, abnormalities of the brain and spinal cord and others...
- Software combined conversion of the resulting risk of possible disability of the foetus with Down Syndrome and another chromosomal aberration using FMF (Fetal Medicine Foundation) certified software Astraia©. We will notify you of the results by postal mail or in the case of positivity of the test on the next day working after your examination.
If the value of risk of a foetus affected by Down Syndrome and another chromosomal aberration is:
- >1:4 až 1:300 is high risk, and you will have recommended invasive prenatal diagnostics, i.e. chorionic villus sampling (CVS) for determining the chromosomal makeup of the foetus with a result within 24 to 48 hours. According to your preference it is also possible to carry out a non-invasive examination of cell-free foetal DNA (cffDNA) from your blood – PRENASCAN.
- 1:301 až 1:1000 is medium risk, and you will be recommended to undergo ultrasound examination in weeks 18-20 of pregnancy – genetic ultrasound with recalculation of the risk
- <1:1000 is low risk, and we recommend ultrasound morphological examination in weeks 19-23 of pregnancy
What is it for?
The combined test is the most effective screening method for chromosomal aberrations and morphological abnormalities in relation to applicability and recovery (high specificity and sensitivity) in early pregnancy. At the same time it significantly lowers the necessity of an invasive diagnostic procedure in women as well as chorionic villus sampling and amniocentesis and in contrast it increases the capture of Down Syndrome and other chromosomal abnormalities to more than 95%-98%.
Vyšetrujúci lekár musí byť každoročne auditovaný pod hlavičkou the Fetal Medicine Foundation a certifikovaný pre jednotlivé ultrazvukové merania (nuchálna translucencia – NT, nosová kosť – NB, trikuspidálna regurgitácia – TR, ductus venosus – DV). Dané ultrazvukové vyšetrenie kladie vysoké nároky aj na samotnú kvalitu ultrazvukového prístroja v CFGD je to rodina high-end expertných prístrojov Voluson od firmy GE. Vyšetrenie voľného ß-hCG a PAPP-A z krvi matky musí byť prevádzané v akreditovanom laboratóriu. Výsledné individuálne riziko Downovho syndrómu musí byť kalkulované len v programe, ktorý vypočítava dané riziko cez algoritmus založený na vedeckých podkladoch FMF, t.j. Astraia© alebo ViewPoint©.
It is important to be aware that ultrasound NT measuring itself has only a 70-80% detectability for Down Syndrome versus 95-98% with the combined test. NT measuring, however, requires certification and auditing of results by the FMF foundation.
How is Down Syndrome diagnosed?
The combined test does not diagnose Down Syndrome itself, but it offers the client the individual risk for this possible disability. To have the capability to assess its risk factor in the early phase of pregnancy helps you and your gynecologist to effectively make the right decision. A definitive answer i.e. diagnosis of Down Syndrome or another chromosomal aberration, can be made only by genetic examination of foetal or placental cells. This is either CVS (chorionic villus sampling) or AMC (sampling of amniotic fluid, amniocentesis) examinations.
Is it possible to determine schistorrhachis early?
Recently, a new marker, the so-called IT (intracranial translucence), which deals with the risk of the foetus having an opening on the spinal cord – NTD (neural tubal defect) has been added to the morphological examination in the first trimester. This marker shifts the diagnosis of NTD from the period of the second to the first trimester. This examination is based on ultrasound observation of the individual sonomorphological parts of the 4 brain chambers with subsequent evaluation by IT, which is absent with congenital open schistorrhachis.









II. trimester
Morphological and genetic ultrasound
Generally
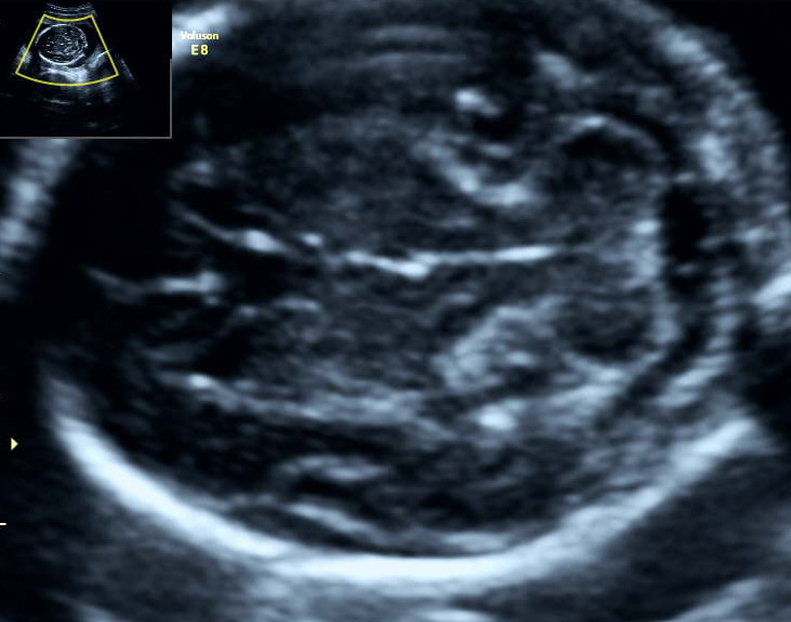
The most important ultrasound examination for excluding congenital developmental birth defects. It evaluates in detail the anatomy and captures the majority of abnormalities of internal organs in the body of the foetus. In the case of the heart and kidneys it’s possible to make determinations also regarding their function. We measure the size of the individual parts of the foetus – typically the diameter and circumference of the head (biparietal diameter - BPD, HC), abdominal circumference (AC) and the length of the leg and arm bones (FL, HL) – by which we assess adequate growth of the foetus. The status of location of the placenta is also evaluated as well as the amount of amniotic fluid, the cervix with possible Doppler metric measurements of the veins of the foetus and mother.
Genetic ultrasound consist of searching for and evaluating defects/anomalies of so-called markers, which often occur in foetuses with chromosomal aberrations (Down, Edwards, Patau Syndrome and others). Such an examination by ultrasound increases the detection of foetuses with Down Syndrome and significantly lowers the necessity of invasive amniocentesis. The aim of genetic ultrasound is to assign to each patient individually – her own risk – for a possible foetus with Down Syndrome and not only general risk derived from the age of the patient or a calculation on the basis of biochemical screening (triple test, double test, serum integrated test...). Detectability of Down Syndrome by genetic ultrasound achieves 91%, whereas with a basic clinical morphological ultrasound this is only 50%.
When?
Morphological ultrasound examination of the foetus is done in the second trimester of pregnancy as a so-called second-trimester ultrasound screening between weeks 19 and 22 of the pregnancy. We perform genetic ultrasound between the 18th to 20th weeks of pregnancy; the given limitation of weeks is linked to the capturing of individual sonograph markers and for potential time possibility of genetic examination either NIPT analysis (link to PRENASCAN) or amniotic fluid – amniocentesis (link to AMC).
How?
We most often carry out the examination with a USG abdominal probe. Before the examination we ask that you empty your urinary bladder and not apply any creams to the abdomen. Always bring all ultrasound findings from your pregnancy as well as other medical documentation with you. Genetic ultrasound is conceived as a second-trimester screening for increasing the capture of foetuses in which chromosomal aberrations are suspected. The idea has found wider application in the USA in particular. Here in Central Europe it is fully substituted by the first-trimester combined test and morphological ultrasound. If, however, a client has not undergone the mentioned screening approach, genetic ultrasound offers the opportunity for negating a positive biochemical screening for Down Syndrome without the need for amniocentesis or NIPT. Here at CFGD we annually negate by genetic ultrasound more than 95% of “triple tests” positive for Down Syndrome. For exact calculation of the risk of chromosomal aberration it is essential that the patient bring the result of a biochemical screening with her.
What is it for?
Basic morphological ultrasound is a standard anatomical examination of the foetus (SSUM recommendation for prenatal examinationand according to these recommendations it is done in the majority of primary gynecological clinics. This standard ultrasound examination is therefore useful, but with respect to its simplicity it has notably specific limitations for the detection of congenital defects.
Expanded morphological ultrasound, which we perform at CFGD, is supplemented compared to basic morphological ultrasound by these examinations:
- detection of minor markers for chromosomal aberrations
- examination of the heart beyond the framework of four-chamber projection
- expanded neurosonogram of individual parts of the foetal brain
- colour, pulsed and tissue Doppler metric measurement
- application of 3D/4D ultrasound modalities
- syndromological detection
- Practice guidelines for performance of the routine mid-trimester fetal ultrasound scan
- ISUOG Practice Guidelines (updated): sonographic screening examination of the fetal heart
- Sonographic examination of the fetal central nervous system: guidelines for performing the ‘basic examination’ and the ‘fetal neurosonogram’
- Screening for chromosomal defects (Nicolaides KH, Screening for chromosomal defects, editorial. Ultrasound Obstet. Gynecol. 2003 Apr;21:313-21.)
- Genetic sonography – the historical and clinical role of fetal echocardiography
- ACR–ACOG–AIUM–SMFM–SRU PRACTICE PARAMETER FOR THE PERFORMANCE OF STANDARD DIAGNOSTIC OBSTETRICAL ULTRASOUND
- Content of a complete second trimester obstetrical ultrasound








III. trimester
Screening for growth retardation of the foetus and examination of flows
Generally
We perform ultrasound screening of early inter-uterine growth retardation (early IUGR) of a foetus between the 28th and 32nd weeks and later inter-uterine growth retardation (late IUGR) after the 32nd week of pregnancy.
- growth and weight of the foetus
- amount of amniotic fluid
- prietoky v srdcovocievnej cirkulácii plodu a medzi maternicou a placentou
- position and state of the placenta
- movements of the foetus
- additional diagnosis, or monitoring of congenital defects
When?
Skríning rastovej retardácie plodu a vyšetrenie prietokov je najlepšie podstúpiť už na začiatku tretieho trimestra tehotenstva (28-32 týždeň gravidity). Výsledok tohto vyšetrenia pojednáva o stave plodu, vyhodnocuje jeho rast a prietoky krvnej cirkulácie, ktoré poukazujú na možné hypoxické ohrozenie plodu a riziko preeklampsie. V skratke toto vyšetrenie hodnotí “ako dobre sa má plod” (fetal well being scan) a či existuje pre pacientku zvýšené riziko preeklampsie (pôvodne gestóza). Tento typ ultrazvukového vyšetrenia sa v prípade podozrenia na závažné ohrozenie plodu vykonáva už pred 20 týždňom gravidity.Genetický ultrazvuk realizujeme medzi 18 až 20 týždňom tehotenstva, daná limitácia týždňov je viazaná k záchytu jednotlivých sonografických markerov a pre prípadnu časovú možnosť genetického vyšetrenia, buď analýzou NIPT (PRENASCAN) alebo plodovej vody – amniocentéza (AMC).
How?
We carry out the examination most often with an abdominal USG probe. During the examination the patient lies on her back or turned slightly on her left side, thus reducing the risk of vena cava inferior syndrome.
What is it for?
with calculation of its estimated weight relevant to the week of pregnancy and projection to a current percentile graph. We focus on a foetuses with insufficient growth, which are under the 10th percentile on the growth graph for the given week of pregnancy. These make up 10% of the group of all foetuses and together they are labelled as “Foetal Growth Restricted - FGR”. It is FGR foetuses that require increased monitoring. More than 30% of FGR foetuses are affected by so-called Intrauterine Growth Restriction – IUGR. An IUGR foetus is significantly endangered by birth and pre-birth mortality and morbidity due to long-term haemodynamic adaptation. This arises especially in consequence of an insufficient placenta, which we register by measuring flows. Subsequently, a metabolic adaptation of the foetus develops due to the mentioned changes and the “foetus doesn’t awake and its growth slows.” The purpose of the screening for growth retardation is to capture and monitor IUGR foetuses which are, compared with appropriate for gestational age (AGA) foetuses, endangered to a higher measure by:
- intrapartum asphyxiation
- new-born hypoglycaemia and hypocalcaemia
- aspiration of the meconium
- late psychomotor development
- haemodynamic instability, which leads to right-side heart failure
which enables the assessment of the functional state of the foetus in the uterus. The first reaction of a foetus to a lowered input of nutrients from the placenta is a lowering of the metabolic needs of the foetus, which leads to a slowing of growth. At the same time flow is increased in the cerebral stream, which is the first flow sign of compensation. Cerebral flow achieves a maximum perhaps two weeks prior to the start of slowing of heart frequency. But the redistribution of changes in circulation of a foetus continues up to birth. With reduced input of oxygen and nutrients from the placenta, the foetus with the help of blood circulation redistribution ensures sufficient arrival of oxygen and nutrients to the brain, heart muscles and adrenal glands. While the foetus is capable due to this compensation mechanism to preferentially ensure oxidation of the myocardia, it is not able to develop the right side of the heart. Therefore, the majority of foetuses in which Doppler metric measurement demonstrates arterial redistribution with normal venal flow has in this phase normal, reactive heart activity curves during cardiovascular examination – CTG. Doppler metric measurement, compared with CTG examination, is capable of pointing to distress of the foetus up to four-weeks in advance. Examination of flows consists of Doppler metric assessment of the blood vessels of the uteroplacental (uterine arteries – AUt) and the foetal (umbilical blood vessels – AU and VU, middle cerebral artery – MCA, the aortal isthmus – AoI and the ductus venosus - DV) circulation.









pre objektivizáciu slúži stanovenie jej indexu AFI – Amniotic Fluid Index. Index vyjadrený v dĺžkových jednotkách centimetroch (cm) vyhodnocuje veľkosť štyroch najväčších priestorov s plodovou vodou v štyroch určených maternicových lokalitách. Táto metóda umožňuje porovnanie množstva plodovej vody s odstupom času. Pokles indexu množstva plodovej vody môže signalizovať plod v kompenzácií alebo pod stresom, ktorý sa prejaví ešte skôr ako zmeny pri kardiotokografickom non-stress teste (CTG/NST). U IUGR plodov sa daný index môže znižovať náhle alebo pomaly.
during which we determine its localization, structure and degree of “maturation”. With growth retardation of the foetus we evaluate the volume of the placental tissue, because IUGR of the foetus shows in terms of volume about 25% smaller placenta than a normal foetus. Likewise, placenta circumvallata, placenta membranacea and a placenta with chorangiomatosis occur in a higher measure in these foetuses. The most significant cause of development of IUGR is insufficient placenta tissue, especially abnormal changes in the terminal villous compartment.
we examine and determine these with each ultrasound examination. We conduct a more detailed focusing on the types of movements with evaluations of a biophysical profile of the foetus using 2D eventual 3D/4D modes. Experimental examination of foetal movements using the KANET test (3D/4D sonography) can help with identification of the disability of a foetus with children’s cerebral palsy.